Tendon repair techniques have advanced, yet failure rates remain a challenge, especially in high-demand or biologically compromised patients. While fixation has improved, biology—not just mechanics—often determines long-term success.
👉 When should you augment a tendon repair—and how does it impact the biologic environment?
This guide highlights key clinical applications across the knee and foot & ankle, with an emphasis on optimizing the biologic environment for healing.
The Biologic Gap in Tendon Healing
Tendon-to-bone healing is inherently complex. Even with strong fixation, healing often occurs through scar tissue rather than native enthesis, which can compromise durability (Pugliese et al., 2024).
Common challenges:
- Poor vascularity
- Limited cellular activity
- High mechanical stress
- Degenerative tissue
Augmentation, when used effectively, helps optimize the biologic environment—not just reinforce the repair.
Not All Augmentation Is Created Equal
Many solutions—especially collagen-based products—act as onlay patches, supporting the tendon surface but not necessarily the tendon-to-bone interface, where failure often occurs.
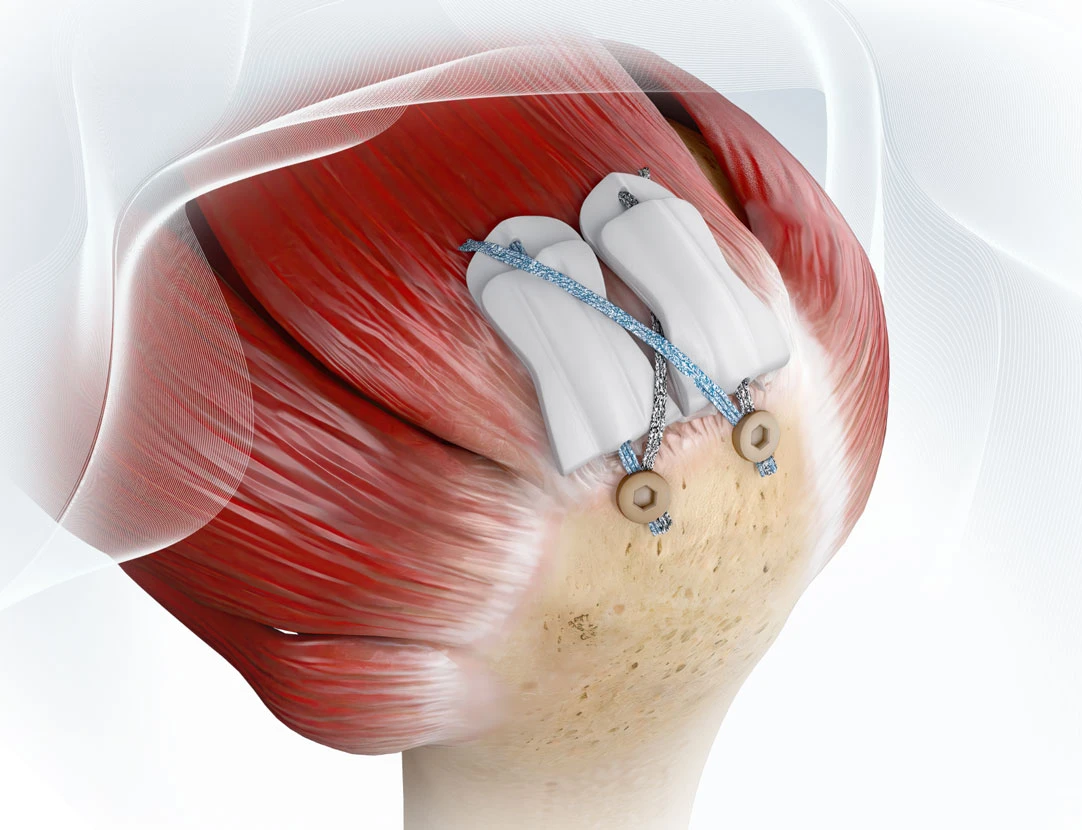
In contrast, synthetic scaffolds, such as ROTIUM® Bioresorbable Wick are designed to:
- Sit at the repair interface (interpositional) or wrap around a tendon (management and protection of the tendon)
- Retain biologic factors at the site
- Drive healing through chemical mediators from the synthetic polymers, PGA & PLCL
- Support cellular organization and native remodeling
It’s important to consider not just when to augment, but how it influences healing.
When to Consider Augmentation
Augmentation is commonly considered in:
- Poor tissue quality: degeneration, revision
- High-tension repairs: risk of failure
- Revision cases: compromised biology
- High-demand patients: athletes
- Biologic risk factors: comorbidities such as age, smoking, diabetes
Knee Applications
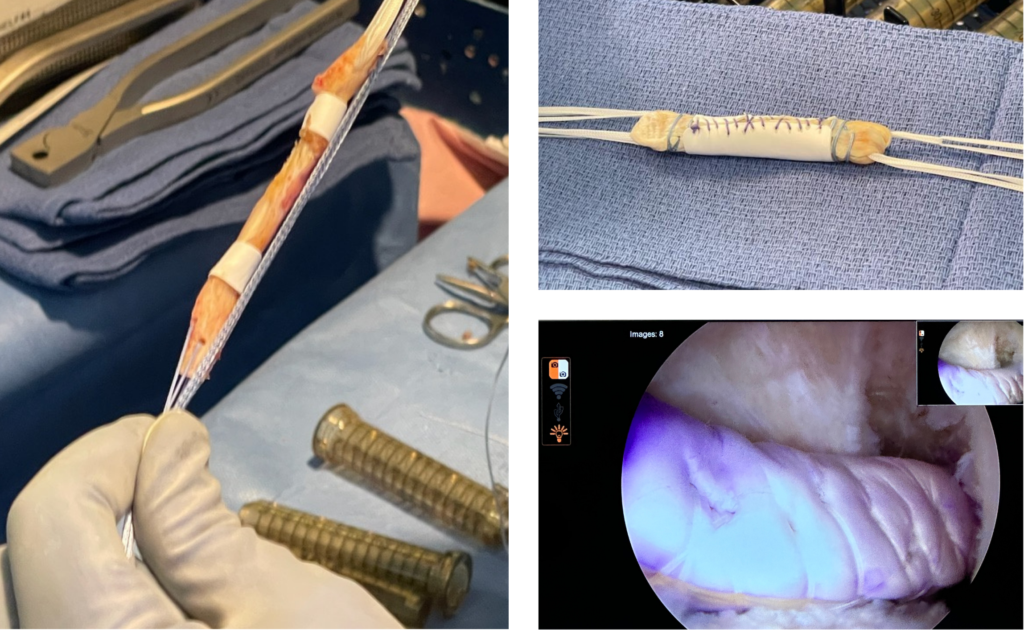
In the knee, augmentation is most relevant in tendon repairs under high load. In ACL reconstruction, for example, some surgeons are exploring the use of interpositional scaffolds, such as ROTIUM®, placed around the graft within the tunnel to support the biologic environment at the tendon-to-bone interface.
Other common scenarios:
- Patellar tendon repair
- Quadriceps tendon repair
- Complex or multi-structure injuries
- ACL Reconstruction
Consider augmentation when:
- Tissue quality is poor
- Repair tension is high
- Revision or chronic injury is present
In these settings, strategies that emphasize biologic environment optimization at the interface may be particularly valuable.
Foot & Ankle Applications
Foot & ankle procedures face high loads and biologic limitations, making healing less predictable.
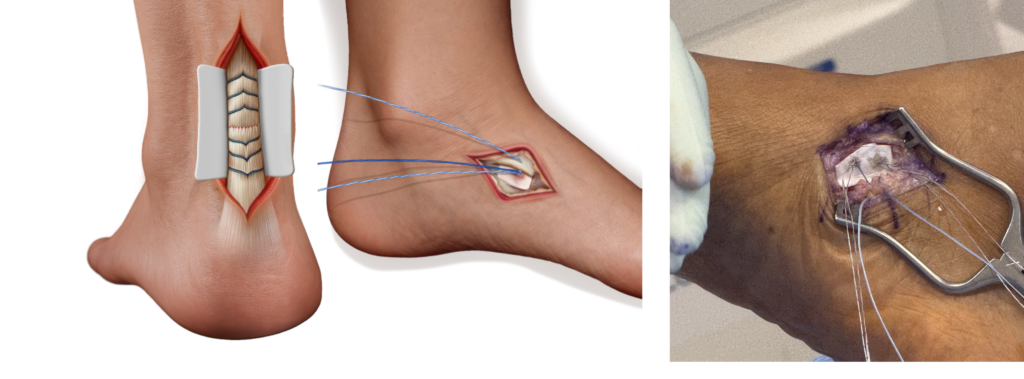
Achilles Tendon Repair
- Limited vascularity
- High biomechanical demand
Consider augmentation in:
- Chronic ruptures
- Large defects
- Revision cases
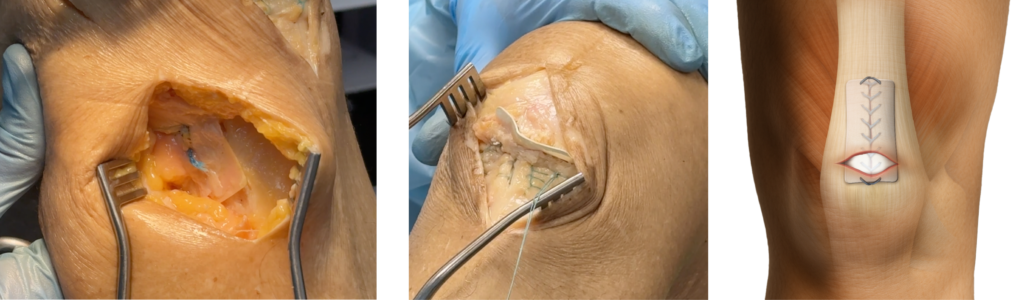
Kidner Procedure
Relies on tendon-to-bone integration
Augmentation may support:
- Interface healing
- Compromised tissue quality
Applying Augmentation Through Biologic Environment Optimization
Augmentation is shifting from structural support to biologic strategy.
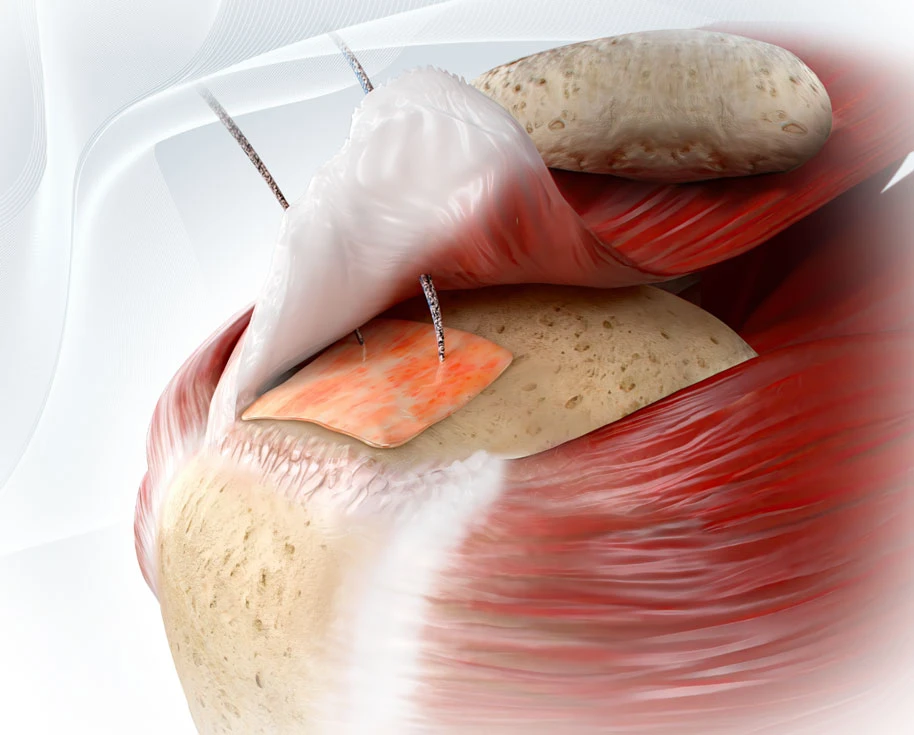
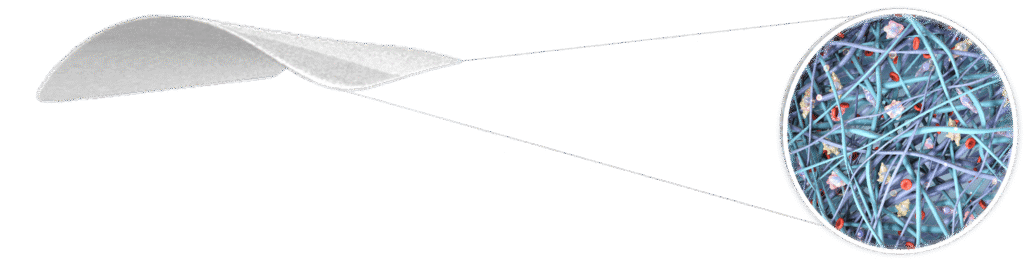
Technologies like ROTIUM® bioresorbable scaffold function as an interpositional wick, placed at the repair interface to:
- Retain the patient’s own biologic factors
- Provide a nanofiber matrix similar to native ECM
- Support organized tissue healing
This shift—from augmenting repairs to influencing how healing occurs—is becoming increasingly relevant across knee and foot & ankle procedures. Success depends not only on when augmentation is used, but how it supports the biologic environment at the tendon-to-bone interface. Ultimately, the quality and durability of healing are driven as much by biology as by fixation.
References
- Pugliese E, et al. Tendon-to-bone healing: current challenges and emerging strategies. Biomaterials Advances. 2024;157:213740.
- Bishnoi A, Bhatia M. Current Concepts in Acute Achilles Tendon Injury. Journal of Foot and Ankle Surgery (Asia Pacific). 2022;9(3):130–134.
- Maffulli N, et al. Current concepts review: Achilles tendon rupture. Journal of Bone and Joint Surgery Am. 2011;93(11):1075–1088.